The process of FDF involves with varying degrees, seven steps. Though they look like steps following a straight line, they are interlinked back to information gathering.
This requires being close to the target group. Issues are various constraints or challenges that the target group faces. The biggest challenge of our time is HIV/AIDS. It is a disease that is taking away human life. It persists despite threatening to wipe away whole populations It is the main concern of every person in the world today. Issues come out of discussion with leaders, observation and listening to local people.
The focus of TDF in relation is on behaviour change in communities. The concept of community carries the meaning of people living together and sharing common values. In order to know what behaviours, practices and values that have contributed to the spread of HIV/AIDS, you need to have a broad picture that should include i) recent History in relation to HIV/AIDS ii) Behaviours, Practices and values that contribute to the spread of HIV/AIDS iii) impact of HIV/AIDS at household level.
All these aspects of the broader picture become clear when you embark on information gathering. To gather information, you can use research tools. The tools for researchers include questionnaires, interviews etc. The research tools you are going to learn more about are those embodied in participatory learn approaches and interviews. The PLA tools are much easier to understand and apply. Though they look simple, they are scientific tools in their approach because they help the researcher to collect information in a systematic way. You should begin gathering information within the group and later move into the community.
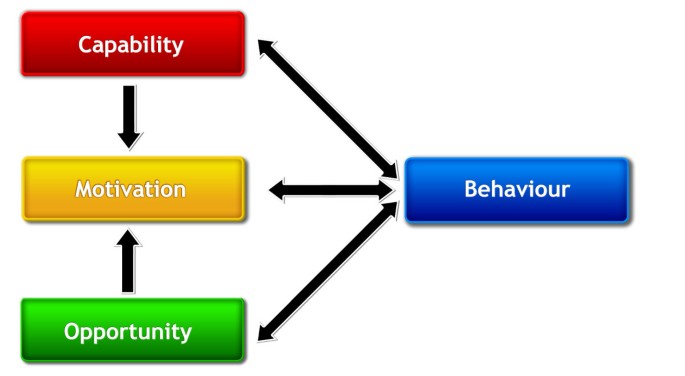
In development work you are concerned with effecting some change in behavior and attitudes. Without promoting change nothing happens. But change in not easy. It requires patience and skill in dealing with human beings. Kebaabetsare and Norr (2002) have stated that understanding the behaviours that put people at risk of contracting HIV and identifying ways of changing such behaviours is a sure way of stopping the spread of HIV in Africa and other developing Countries.
The ABC (Abstinence, being faithful and condom' use, are recognized as positive behaviours that can reduce the spread of HIV.
a) Abstinence - this involves delay of sexual experience especially for adolescents
b) Being faithful — sticking to one sexual partner or reducing the number of sexual partners
Condom use: Effective use of condoms. This is more effective among Commercial Sex Workers (CSWs). Sometimes distribution of condoms to school-going children has aroused opposition. The Minister of Education in Zambia has banned distribution of condoms in schools
i. Epidemiologic Approaches
Targets high risk groups such as CSWs, Injection Drug Users (IDUs), men having sex with men and Lesbians, adolescents, young adults and women, can be cost effective and efficacious (efficient)
b) Holistic Approach
Targets the general population
This could help in reducing stigma because it targets every one. It can also gain political support because it is popular. One weakness is that it can be costly- spread of resources rather thinly.
There are two broad methodological approaches each with specific models to behaviour change:
a) Small/ individual group models — These focus on understanding and explaining were change can take place in individuals and in small groups.
i) Health beliefs model: This identifies four key beliefs or perceptions to behaviour change as:
a) Threat — when people see threat they can change
b) Efficacy (Self Confidence) and benefits
c) Barriers or negative effects —these have to be identified
d) Cues to action - e.g Mass campaigns
ii) Theory of reasoned action model: This identifies the intention in people as the route to change. Intention is influenced by:
a) perceived outcomes
b) evaluation of outcomes or social norms (especially expectation). Efficiency rehearsal and support
c) Increasing self-efficacy through identifying modeling.
iii) integrated social learning model: identifies the following as key to behaviour change.
a) Positive Cost/benefit ratios
b) Strong Intent
c) Necessary skills
d) High self -efficacy (self-confidence)
e) Expected positive emotional response
f) Compatibility of behaviour with self-image
g) Greater perceived social pressure to perform a behaviour than not to perform
h) Fewer environmental constraints to perform a behaviour than not performing
iv) The AIDS risk reduction model: there are three basic steps
a) Labeling one's own behaviour as risky
b) Making a commitment to reducing risk behaviour
c) Taking action to perform the desired change.
v. Trans-theoretical Model identifies four steps:
i. precontemplation
ii. contemplation
iii. action
iv. maintenance
b) Community/ Societal models:
Directed at entire communities and aims at making structural
changes.
Different approaches/theories which support this include
i) Diffusion of Innovation theory — change is brought about by innovators i.e influential people. This relies on use of peer educators
ii) Mass media campaign
-Use of Video, TV dramas posters and mass rallies
iii) Community Empowerment Approach — also called Community organization, Community mobilization, Action research. Community empower,ment approach addresses behaviour broadly and actively involves community members in designing, executing and evaluating the project
iv) Social Marketng — uses commercial methods to promote behaviour change. The marketing of condoms in Zambia through advertisements is an example of social marketing. It involves structural change because it changes social norms and reduces structural barriers
v) Policy or infrastructure changes — these are policy changes that affect structures e.g distribution of condoms to all sex workers
1) Economic barriers
· Poverty - leads to sex work
· Migrant work separates families. When away, migrant workers turn to CSW. The spouses who remain behind engage in extra marital sex.
· Prolonged separation due to studies
· Migration i.e due to famine and political conflicts
2) Social and Cultural barriers
· Stigma and denial. Stigma is characterized by:
- fear to discuss the disease
failure to recognize personal risk
- prevention or reluctance to learn or disclose HIV/Status
In Zambia the major problem is stigma. The Zambia millennium goals report singles out stigma, attitude and misconceptions as major health and economic challenges (Republic of Zambia 2003: 24) stigma involves
· Familial concealment (hiding) of HIV status and AIDS related deaths
· Not discussing sexuality openly except during traditional initiation rites
· Parents not willing to educate children on about HIV transmission
· Rejection of sex education in schools
· Women having limited power to negotiate safer sexual practices due to lack of economic, political power
· Polygamy
3) Organizational barriers
· Competition over resources
· Not evaluating behaviour change interventions to establish comparative advantage
4) Political barriers
· Weak, unstable governments
· Armed conflict and health crises
· Wide spread misinformation denial and stigma
· Lack of policies on poverty reduction
· Lack of political will at high level of state power.
You are going to identify institutions that support or work with people affected or infected with HIV/AIDS. To be affected is to suffer as a result of another person being a patient of HIV/AIDS. When parents are sick, children are affected. They are deprived of the care they used to receive because the parents are not able to do all those things they used to do such as working to fend for the family.
To be infected is to carry HIV/AIDS in the body. People that are sick are said to be living with HIV/AIDS. Due to the concern that HIV/AIDS has created, nations and the international community have responded by creating institutions large and small, local and international, that give support to the affected and infected.
You have now collected and analyzed information in different groups. Information you have put on flip charts covers I) recent history using time lines ii) Behaviours, values and attitudes that contribute to spread of HIV/AIDS using matrices iii) Institutions that support those infected using venn diagrams and iv) impact of HIV/AlDs at household level using maps. The use of PLAs instantaneously leads to issue analysis. At the end you are required to create composite tools to give greater validity to the findings through intergroup PLA agreement.
Now that you have collected information from among yourselves, you will go into the field and collect further information. Field work requires preparation in terms of i) methods of collecting information ii) preparing the people to receive you iii) gaining entree in the community
a) Methods of collecting information. You can use PLAs to go and collect information from the community. In fact extension of PLAs to the communities increases group participation. That you are quite skilled to use PLAs, you will look at the use of interviews to collect information. Interviews are suitable for collecting information from individuals. There are three types of interviews: 1) unstructured, semi structured and structured interview.
Unstructured Interviews
Unstructured Interviews are also referred to as clinical interviews. Questions are not written and interviews arise from conversations. A conversation is a discussion with a purpose. These interviews flow from asking grand tour questions. They would involve asking questions like "how long have you been here'?" 'Tell me what do you normally do in your life to earn a living". Questions of this nature are designed to ease the atmosphere and to bring the researcher and the researched closer. There is also need for the researcher to make a deliberate effort to stop and let the interviewee ask some questions. Unstructured interviews can unlock new and often unintended discoveries.
Semi-Structured Interviews
Semi-structured interviews these are interviews which follow preformed questions. At the beginning, you prepare a series of questions to guide the interview. Questions can be asked in a different order as the interview proceeds when you ask the interviewee one question but in answering the first question interviewee answer also question two, in that case do not repeat question two. Interviews can be recorded or written down. If recorded, it is advisable to use a small tape recorder with an in built microphone. The recorder can be an obstruction to free and natural conversations for a varying length of time. Awareness of the machine can cause some uneasiness on the part of the interviewee. It is good for the researcher to talk about the recorder. If no explanation is given for presence of a tape recorder, the interviewee can remain apprehensive about its presence. If an explanation is made and permission sought awareness of its intrusion may not last long. One way of making a recorder interviewee-friendly is to play back a short part of the conversation that has taken place in the first five also minutes of each interview. A researcher can say something like "let us listen to what we have recorded so far". The listening can provide the interviewee with extra courage and confidence as well as ease tensions.
Structured Interview
Structured interview is a set of carefully worded questions. The questions are arranged under subheadings of the topic under investigation and are asked of interviewees in the same order. For example, in an investigation on listening to the girl child questions were arranged under the subheadings: aspirations and expectations, family expectations and class interactions.
Introduction
The term process carries the meaning of series of actions, tasks or steps that are taken to achieve something. In theatre for developmentthat something is increasing participation of the people that animateurs work with so that they can make change in their lives. The change that takes place in the lives of target group is what becomes education.
| The Research Process in Theatre For Development |
Table of Contents
The process of FDF involves with varying degrees, seven steps. Though they look like steps following a straight line, they are interlinked back to information gathering.
This requires being close to the target group. Issues are various constraints or challenges that the target group faces. The biggest challenge of our time is HIV/AIDS. It is a disease that is taking away human life. It persists despite threatening to wipe away whole populations It is the main concern of every person in the world today. Issues come out of discussion with leaders, observation and listening to local people.
The focus of TDF in relation is on behaviour change in communities. The concept of community carries the meaning of people living together and sharing common values. In order to know what behaviours, practices and values that have contributed to the spread of HIV/AIDS, you need to have a broad picture that should include i) recent History in relation to HIV/AIDS ii) Behaviours, Practices and values that contribute to the spread of HIV/AIDS iii) impact of HIV/AIDS at household level.
All these aspects of the broader picture become clear when you embark on information gathering. To gather information, you can use research tools. The tools for researchers include questionnaires, interviews etc. The research tools you are going to learn more about are those embodied in participatory learn approaches and interviews. The PLA tools are much easier to understand and apply. Though they look simple, they are scientific tools in their approach because they help the researcher to collect information in a systematic way. You should begin gathering information within the group and later move into the community.
In development work you are concerned with effecting some change in behavior and attitudes. Without promoting change nothing happens. But change in not easy. It requires patience and skill in dealing with human beings. Kebaabetsare and Norr (2002) have stated that understanding the behaviours that put people at risk of contracting HIV and identifying ways of changing such behaviours is a sure way of stopping the spread of HIV in Africa and other developing Countries.
The ABC (Abstinence, being faithful and condom’ use, are recognized as positive behaviours that can reduce the spread of HIV.
a) Abstinence – this involves delay of sexual experience especially for adolescents
b) Being faithful — sticking to one sexual partner or reducing the number of sexual partners
Condom use: Effective use of condoms. This is more effective among Commercial Sex Workers (CSWs). Sometimes distribution of condoms to school-going children has aroused opposition. The Minister of Education in Zambia has banned distribution of condoms in schools
i. Epidemiologic Approaches
Targets high risk groups such as CSWs, Injection Drug Users (IDUs), men having sex with men and Lesbians, adolescents, young adults and women, can be cost effective and efficacious (efficient)
b) Holistic Approach
Targets the general population
This could help in reducing stigma because it targets every one. It can also gain political support because it is popular. One weakness is that it can be costly- spread of resources rather thinly.
There are two broad methodological approaches each with specific models to behaviour change:
a) Small/ individual group models — These focus on understanding and explaining were change can take place in individuals and in small groups.
i) Health beliefs model: This identifies four key beliefs or perceptions to behaviour change as:
a) Threat — when people see threat they can change
b) Efficacy (Self Confidence) and benefits
c) Barriers or negative effects —these have to be identified
d) Cues to action – e.g Mass campaigns
ii) Theory of reasoned action model: This identifies the intention in people as the route to change. Intention is influenced by:
a) perceived outcomes
b) evaluation of outcomes or social norms (especially expectation). Efficiency rehearsal and support
c) Increasing self-efficacy through identifying modeling.
iii) integrated social learning model: identifies the following as key to behaviour change.
a) Positive Cost/benefit ratios
b) Strong Intent
c) Necessary skills
d) High self -efficacy (self-confidence)
e) Expected positive emotional response
f) Compatibility of behaviour with self-image
g) Greater perceived social pressure to perform a behaviour than not to perform
h) Fewer environmental constraints to perform a behaviour than not performing
iv) The AIDS risk reduction model: there are three basic steps
a) Labeling one’s own behaviour as risky
b) Making a commitment to reducing risk behaviour
c) Taking action to perform the desired change.
v. Trans-theoretical Model identifies four steps:
i. precontemplation
ii. contemplation
iii. action
iv. maintenance
b) Community/ Societal models:
Directed at entire communities and aims at making structural
changes.
Different approaches/theories which support this include
i) Diffusion of Innovation theory — change is brought about by innovators i.e influential people. This relies on use of peer educators
ii) Mass media campaign
-Use of Video, TV dramas posters and mass rallies
iii) Community Empowerment Approach — also called Community organization, Community mobilization, Action research. Community empower,ment approach addresses behaviour broadly and actively involves community members in designing, executing and evaluating the project
iv) Social Marketng — uses commercial methods to promote behaviour change. The marketing of condoms in Zambia through advertisements is an example of social marketing. It involves structural change because it changes social norms and reduces structural barriers
v) Policy or infrastructure changes — these are policy changes that affect structures e.g distribution of condoms to all sex workers
1) Economic barriers
· Poverty – leads to sex work
· Migrant work separates families. When away, migrant workers turn to CSW. The spouses who remain behind engage in extra marital sex.
· Prolonged separation due to studies
· Migration i.e due to famine and political conflicts
2) Social and Cultural barriers
· Stigma and denial. Stigma is characterized by:
– fear to discuss the disease
failure to recognize personal risk
– prevention or reluctance to learn or disclose HIV/Status
In Zambia the major problem is stigma. The Zambia millennium goals report singles out stigma, attitude and misconceptions as major health and economic challenges (Republic of Zambia 2003: 24) stigma involves
· Familial concealment (hiding) of HIV status and AIDS related deaths
· Not discussing sexuality openly except during traditional initiation rites
· Parents not willing to educate children on about HIV transmission
· Rejection of sex education in schools
· Women having limited power to negotiate safer sexual practices due to lack of economic, political power
· Polygamy
3) Organizational barriers
· Competition over resources
· Not evaluating behaviour change interventions to establish comparative advantage
4) Political barriers
· Weak, unstable governments
· Armed conflict and health crises
· Wide spread misinformation denial and stigma
· Lack of policies on poverty reduction
· Lack of political will at high level of state power.
You are going to identify institutions that support or work with people affected or infected with HIV/AIDS. To be affected is to suffer as a result of another person being a patient of HIV/AIDS. When parents are sick, children are affected. They are deprived of the care they used to receive because the parents are not able to do all those things they used to do such as working to fend for the family.
To be infected is to carry HIV/AIDS in the body. People that are sick are said to be living with HIV/AIDS. Due to the concern that HIV/AIDS has created, nations and the international community have responded by creating institutions large and small, local and international, that give support to the affected and infected.
You have now collected and analyzed information in different groups. Information you have put on flip charts covers I) recent history using time lines ii) Behaviours, values and attitudes that contribute to spread of HIV/AIDS using matrices iii) Institutions that support those infected using venn diagrams and iv) impact of HIV/AlDs at household level using maps. The use of PLAs instantaneously leads to issue analysis. At the end you are required to create composite tools to give greater validity to the findings through intergroup PLA agreement.
Now that you have collected information from among yourselves, you will go into the field and collect further information. Field work requires preparation in terms of i) methods of collecting information ii) preparing the people to receive you iii) gaining entree in the community
a) Methods of collecting information. You can use PLAs to go and collect information from the community. In fact extension of PLAs to the communities increases group participation. That you are quite skilled to use PLAs, you will look at the use of interviews to collect information. Interviews are suitable for collecting information from individuals. There are three types of interviews: 1) unstructured, semi structured and structured interview.
Unstructured Interviews
Unstructured Interviews are also referred to as clinical interviews. Questions are not written and interviews arise from conversations. A conversation is a discussion with a purpose. These interviews flow from asking grand tour questions. They would involve asking questions like “how long have you been here’?” ‘Tell me what do you normally do in your life to earn a living”. Questions of this nature are designed to ease the atmosphere and to bring the researcher and the researched closer. There is also need for the researcher to make a deliberate effort to stop and let the interviewee ask some questions. Unstructured interviews can unlock new and often unintended discoveries.
Semi-Structured Interviews
Semi-structured interviews these are interviews which follow preformed questions. At the beginning, you prepare a series of questions to guide the interview. Questions can be asked in a different order as the interview proceeds when you ask the interviewee one question but in answering the first question interviewee answer also question two, in that case do not repeat question two. Interviews can be recorded or written down. If recorded, it is advisable to use a small tape recorder with an in built microphone. The recorder can be an obstruction to free and natural conversations for a varying length of time. Awareness of the machine can cause some uneasiness on the part of the interviewee. It is good for the researcher to talk about the recorder. If no explanation is given for presence of a tape recorder, the interviewee can remain apprehensive about its presence. If an explanation is made and permission sought awareness of its intrusion may not last long. One way of making a recorder interviewee-friendly is to play back a short part of the conversation that has taken place in the first five also minutes of each interview. A researcher can say something like “let us listen to what we have recorded so far”. The listening can provide the interviewee with extra courage and confidence as well as ease tensions.
Structured Interview
Structured interview is a set of carefully worded questions. The questions are arranged under subheadings of the topic under investigation and are asked of interviewees in the same order. For example, in an investigation on listening to the girl child questions were arranged under the subheadings: aspirations and expectations, family expectations and class interactions.
This is the Zambian O-level Physics Syllabus Form 1-4, Dec. 2024 version, produced by the…
In this exploration of the math of music, we will delve into how notes and…
This post aims to demonstrate and explain the properties and effects of static electricity, shedding…
Many of the everyday effects of electrostatics involve a charged object losing its charge and…
Area expansion of solids refers to the increase in the surface area of a solid…
The increase in the length of a body resulting from being heated is known as…
{kind=link}
Leave a Comment